NIMHANS Takes on the Stroke Burden with India’s First Endovascular Lab and Homegrown Prototype
India is taking a massive leap forward in battling one of its most stealthy healthcare crises. The National Institute of Mental Health and Neurosciences, better known as NIMHANS, just introduced the country’s very first Endovascular Innovation Laboratory alongside a groundbreaking acute stroke intervention prototype called PARICHAY. Launched in Bengaluru on June 6, 2026, this double-header initiative aims to aggressively reshape how ischemic strokes are managed nationwide. By creating a dedicated hub where researchers, engineers, and clinicians work under one roof, the facility intends to fast-track homegrown medical designs straight from the drawing board to the hospital floor.
For a country dealing with an estimated 1.44 million to 1.66 million new stroke cases every year, the timing couldn't be more critical. The real kicker is that a recent study highlighted by Happiest Health shows one in seven stroke patients in India is under the age of 45, highlighting a terrifying shift toward a younger demographic. When an ischemic stroke hits, a clogged artery chokes off blood to the brain, leaving doctors in a frantic race against the clock. The current gold standard for clearing these blockages relies heavily on expensive mechanical thrombectomy devices imported from Western markets, making life-saving care an elusive luxury for the average citizen.
Breaking the Import Cycle
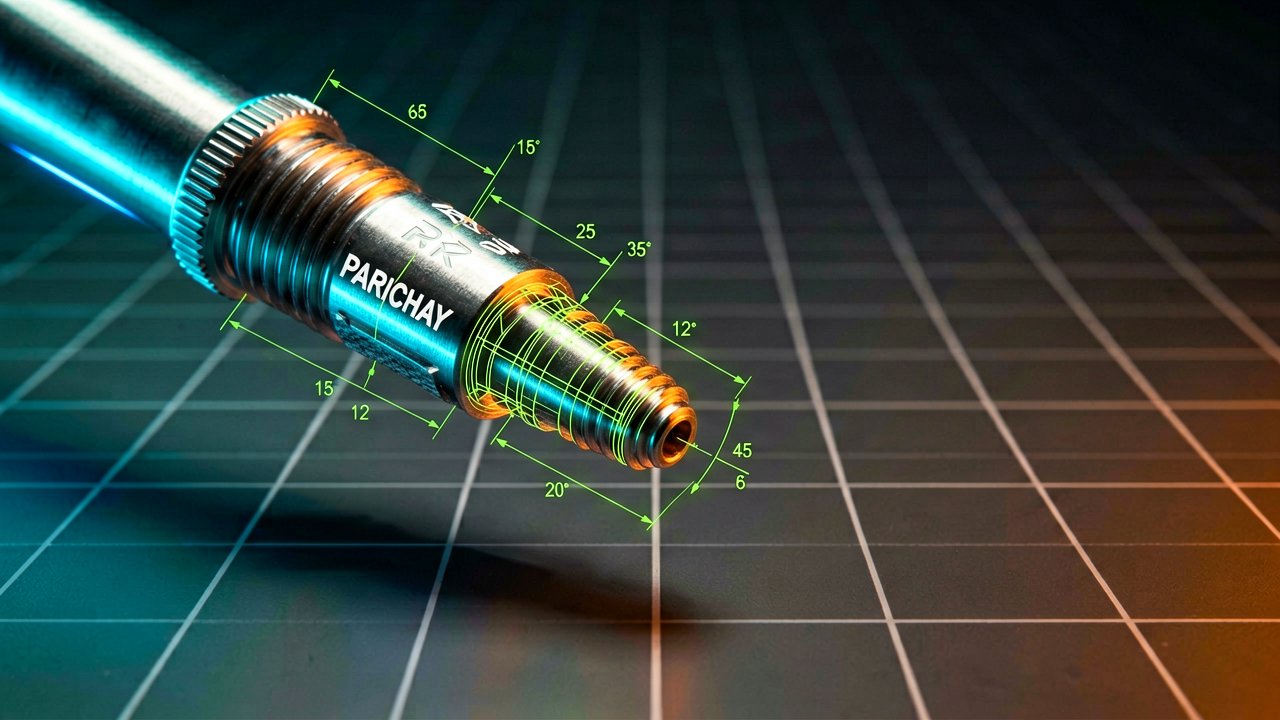
That is where PARICHAY comes in as a potential game-changer. Developed as a homegrown thrombectomy device prototype, it represents a concerted push toward self-reliance in a segment of medical technology historically dominated by multinational giants. Funding for the specialized Endovascular Research and Innovation lab came through the Science and Engineering Research Board and the Anusandhan National Research Foundation, signaling serious state backing for domestic healthtech infrastructure. As reported by The Hindu, the goal isn't just about saving money; it is about building an ecosystem capable of turning local intellectual property into globally competitive clinical tools. By driving down manufacturing and procurement overheads, the initiative could eventually make emergency clot-retrieval procedures standard across tier-2 and tier-3 Indian medical centers.
Of course, a prototype is only the beginning of a incredibly long regulatory journey. PARICHAY will still need to navigate rigorous safety trials and manufacturing scaling before it ever sees real-world emergency room action. However, establishing a dedicated endovascular facility inside a powerhouse institution like NIMHANS ensures that future iterations will be refined by the very doctors performing these procedures daily. It is a vital structural shift, proving that India is no longer content just consuming high-tech medical gear, but is fully intent on designing it.
The Hidden Bottlenecks of Stroke Intervention
Behind the Lab Doors: The true breakthrough of the PARICHAY prototype isn't just its mechanical design, but the structural gridlock it addresses within the Indian healthcare system. For decades, neurointerventionalists in major Indian cities have operated under an unspoken, frustrating reality. They possess the clinical skill to perform life-saving mechanical thrombectomies, but the sheer cost of imported stent retrievers and aspiration catheters—often running into thousands of dollars per procedure—forces a devastating financial choice onto patients' families. Because these devices are single-use and entirely manufactured abroad, hospitals cannot benefit from local economies of scale, effectively keeping advanced stroke care locked behind a steep economic wall.
This economic barrier triggers a cascading crisis of access across the country's geography. While premier institutes in metropolitan areas can maintain inventory, tier-2 and tier-3 hospitals rarely stock these specialized tools due to the high capital risk of expired shelf-life on low-volume, high-cost items. Consequently, a patient suffering an acute ischemic stroke outside a major tier-1 city faces a grim double-jeopardy. They must endure hours of transit time to reach a capable facility, while simultaneously watching the critical golden hour for clot retrieval slip away entirely.
A Paradigm Shift in Medical R&D
By establishing a dedicated space where clinicians sit side-by-side with biomedical engineers, NIMHANS is fundamentally changing how medical hardware is conceptualized in the subcontinent. Historically, Indian medical innovation relied on a fractured model where academic institutions designed theories, private startups scrambled for funding, and manufacturing was outsourced to foreign facilities. This disconnected pipeline frequently resulted in prototypes that looked brilliant on paper but failed to survive the brutal practical realities of a high-pressure corporate medical environment or complex vascular anatomy.
The newly minted Endovascular Innovation Lab bypasses this fragmentation by establishing an immediate feedback loop. When an engineer tweaks the radial force or flexibility of a prototype like PARICHAY, a neurovascular surgeon can immediately test its trackability in synthetic models or anatomical simulators right there in the lab. This tight iterative cycle significantly compresses the traditional multi-year development timeline, allowing developers to spot design flaws, structural weaknesses, or material friction points long before the device ever advances to formal animal or clinical trials.

The Road to Global Benchmarks
However, seasoned medical tech analysts recognize that unveiling a prototype is merely crossing the starting line of an incredibly grueling marathon. For PARICHAY to transition from a celebrated laboratory achievement into a widely trusted clinical tool, it must survive rigorous regulatory scrutiny from the Central Drugs Standard Control Organisation. This pathway demands substantial funding for multi-center clinical trials to prove that the domestic device achieves parity with established international benchmarks in recanalization success rates without introducing higher risks of vascular injury.
Moreover, local manufacturing must scale to meet stringent global quality control standards to ensure that every single unit off the production line behaves identically under immense stress. Stakeholders closely watching the initiative emphasize that if NIMHANS and its state backers can successfully navigate these regulatory hurdles, they will do more than just lower the cost of stroke care in India. They will provide a scalable blueprint for affordable, high-tech medical manufacturing that could easily be exported to other developing nations across the Global South facing identical healthcare disparities.
The Friction Between Innovation and Infrastructure
Reading Between the Lines: The celebration surrounding PARICHAY and the new NIMHANS facility masks a systemic contradiction that tech journalists and healthcare economists routinely overlook. Developing a world-class, cost-effective thrombectomy device inside a state-of-the-art laboratory is an undeniable triumph of Indian engineering, but a device can only save a life if there is an operational theater ready to receive it. The uncomfortable truth is that India’s acute stroke crisis is less about a shortage of intellectual property and far more about a crippling deficit of specialized medical infrastructure and neurointerventional expertise.
Mechanical thrombectomy is not a procedure that can be performed in a standard community clinic; it requires a fully equipped cath lab, advanced digital subtraction angiography imaging, and a highly trained neurointerventional team available 24/7. Currently, these resources are overwhelmingly concentrated in affluent urban corporate hospitals. Introducing a cheaper, homegrown device into this existing ecosystem will undoubtedly pad the profit margins of private hospital networks and lower bills for wealthy patients, but it does fundamentally little to alter the survival odds for a rural patient hours away from the nearest fluoroscopy suite.
The Paradox of Affordability
Furthermore, the assumption that domestic production automatically translates to widespread clinical adoption ignores the entrenched psychology of the medical procurement market. Indian healthcare has long suffered from a prestige bias, where Western regulatory approvals like US FDA clearance or CE markings carry immense institutional weight, often acting as a prerequisite for hospital formulary inclusion. Local innovations, even when backed by robust data from local regulators, frequently face an uphill battle against deep-pocketed multinational giants who use aggressive hospital tied-in contracts, bundled equipment leasing, and extensive physician clinical-education grants to maintain their market dominance.
For PARICHAY to break this cycle, the Indian government will likely need to move beyond merely funding R&D labs and actively intervene in the marketplace. This could mean implementing aggressive domestic procurement mandates in public healthcare schemes or subsidizing the rollout of dedicated stroke centers across underfunded regions. Without these systemic interventions, advanced indigenous medical tech risks becoming a series of prestigious academic trophies—voted as milestones in press releases but left sitting on warehouse shelves while clinicians continue to reach for trusted, imported legacy brands.
Ultimately, the true test of NIMHANS’ ambitious venture will not be found in the sleek architecture of its new endovascular lab or the novelty of its prototype. It will be measured by whether the Indian state can successfully scale the human and physical infrastructure required to deploy these devices where they are desperately needed. Lowering the cost of a device is a brilliant first step, but the harder, far less glamorous work lies in building the widespread clinical network capable of catching a patient before the clock runs out.
Designing a groundbreaking medical device to democratize healthcare is a noble pursuit, provided we ignore the fact that a patient cannot be saved by a wonderfully affordable blood-clot retriever if the nearest cath lab is a four-hour ambulance ride over potholes.
Artūras Malašauskas is an AI Systems Integrator with 20+ years of production-grade web engineering experience. He has designed, shipped, and scaled enterprise Python/PHP systems for logistics, SaaS, and public-sector clients. For the past year, he has focused exclusively on AI integrations: deploying open-source LLMs, building generative media pipelines (image, audio, video), and engineering multi-agent workflows for real production environments. His standard: reproducibility, security, cost-efficient inference—no vaporware. He documents and evaluates emerging AI tooling, separating verified capabilities from marketing noise. Technical editor at: muza-ai.eu, ai-verslas.lt, ai-naujinos.lt Connect on LinkedIn
Comments